Professor Anthony Fryer a.a.fryer@keele.ac.uk

Research Repository
Professor Anthony Fryer a.a.fryer@keele.ac.uk
Adrian Heald
Mike Stedman
Mark B Davies
Martin K Rutter
J. Martin Gibson
Martin Whyte
Aim
Obesity has a significant impact on all-cause mortality rate and overall health care resource use (HCRU). These outcomes are also strongly linked to age, sex and local deprivation of the population. We aimed to establish the lifetime costs of obesity by demographic group/geographic area using published mortality rates and HCRU use for integrated care boards (ICB) in England in the context of costs of therapeutic intervention.
Methods
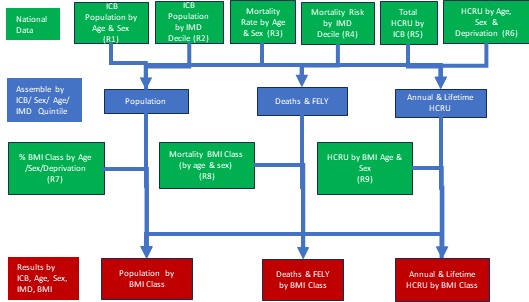
Population and expected mortality rates by age, sex and deprivation were obtained from national data. Obesity class prevalence was taken from the health of the nation study. The published impact of obesity by age, group, sex and deprivation on mortality and HCRU were applied to estimate life years lost and lifetime HCRU [by sex, age band and body mass index (BMI) class for each ICB]. The year 2019 was chosen as the study basis data to avoid influences of COVID-19 pandemic on obesity rates with application of 2022/23 HCRU values. Outcomes including prevalence, deaths, life years lost, HCRU and lifetime HCRU were compared by age and sex groups across four BMI classes normal/underweight (BMI <25 kg/m2), overweight (25-29.9 kg/m2), obese class I and II (30-39.9 kg/m2), and obese class III (≥40), with benchmarking being set against all population being BMI <25 kg/m2 overall and by each of the 42 ICBs. We also associated future life with deaths to provide an estimate of ‘future life years lost’ occurring each year.
Results
Total population aged >16 years was 45.4 million (51% female). Prevalence: 13.7 million (28% of the total adult population) had a BMI ≥30 mg/m2 and BMI ≥40 kg/m2 were 1.50 million (12%) of these 1.0 million (68%) were female and of these 0.6 million 40% were women aged 16-49 years. In addition, 35% of those with a BMI ≥40 kg/m2 were in the top deprivation quintile (i.e. overall 20%). Mortality was based on expected deaths of 518K/year, and modelling suggested that if a BMI <25 kg/m2 was achieved in all individuals, the death rate would fall by 63K to 455K/year for the English population (12% reduction). For those with a BMI ≥40 kg/m2 the predicted reduction was 12K deaths (54% lower); while in those aged 16-49 years with a BMI ≥40 kg/m2 72% of deaths were linked to obesity. For future life years lost, we estimated 2.5 years were lost in people with BMI 30-39.9 kg/m2 6.7 years when BMI ≥40 kg/m2. However, for those aged 16-49 years with a BMI ≥40 kg/m2, 8.3 years were lost. HCRU, for weight reduction, the annual HCRU decrease from BMI ≥40 kg/m2 to BMI 30-39.9 kg/m2 was £342 per person and from BMI 30-39.9 to 25-29.9 kg/m2 the reduction was £316/person. However, lifetime costs were similar because of reduced life expectancy for obese individuals. In quality adjusted life years (QALY), overall, 791 689 future life years were lost (13.1% of all) in people with BMI ≥25 kg/m2 and were related to excess weight. When the NICE £30 000 per QALY value was applied to the estimated total 791 689 future life years lost then the potential QALY value reduction lost was equivalent to £24 billion/year or £522/person in the obese population. For morbidly obese men and women the potential QALY value lost was £2864/person/year. Regarding geography, across the 42 ICBs, we observed significant variation in the prevalence of BMI ≥40 (1.8%-4.3%), excess mortality (11.6%-15.4%) and HCRU linked to higher BMI (7.2%-8.8%). The areas with the greatest impact on HCRU were in the north-west, north-east and Midlands of England, while the south shows less impact.
Conclusion
The expected increases in annual HCRU because of obesity, when considered over a lifetime, are being mitigated by the increased mortality of obese individuals. Our data suggest that simple short-term HCRU reduction brought about through BMI reduction will be insufficient to fund additional specialist weight reduction interventions. The HRCUs associated with BMI are not in most cases related to short-term health conditions. They are a cumulative result over a number of years, so for age 16-49 years reducing BMI from ≥40 to 30-39.9 kg/m2 might show an annual decrease in HCRU/person by £325/year for women and £80/year for men but this might not have immediately occurred within that year. For those aged >70 years reducing BMI from ≥40 to 30-39.9 kg/m2 might show an annual decrease in HCRU/person by £777/year for women and £796/year for men but also may not be manifest within that year. However, for the morbidly obese men and women, the potential QALY value lost was £2864 per person per year with the potential for these funds to be applied to intensive weight management programmes, including pharmacotherapy.
Fryer, A. A., Heald, A., Stedman, M., Stedman, M., Davies, M. B., Rutter, M. K., Gibson, J. M., & Whyte, M. (2024). Counting the Lifetime Cost of Obesity: Analysis based on National England Data. Diabetes, Obesity and Metabolism, 26(4), 1464-1478. https://doi.org/10.1111/dom.15447
| Journal Article Type | Article |
|---|---|
| Acceptance Date | Dec 23, 2023 |
| Online Publication Date | Feb 5, 2024 |
| Publication Date | Feb 5, 2024 |
| Deposit Date | Jan 3, 2024 |
| Publicly Available Date | Feb 6, 2025 |
| Journal | Diabetes, Obesity and Metabolism |
| Print ISSN | 1462-8902 |
| Electronic ISSN | 1463-1326 |
| Publisher | Wiley |
| Peer Reviewed | Peer Reviewed |
| Volume | 26 |
| Issue | 4 |
| Pages | 1464-1478 |
| DOI | https://doi.org/10.1111/dom.15447 |
| Keywords | Obesity, Costs, Mortality, HRCU, Life Years, Life Years Lost, Index of Multiple Deprivation, ICB, QALY |
| Public URL | https://keele-repository.worktribe.com/output/688527 |
Heald Et Al Diabetes Obesity Metabolsim Final Version Dom-23-1557-op-File001
(77 Kb)
Document
Heald Et Al Diabetes Obesity Metabolism 2024 Figures
(42 Kb)
Image
Heald Et Al Diabetes Obesity Metabolsim Final Version Dom-23-1557-op-File001 Tables
(68 Kb)
Document
Monitoring drug interventions in people with bipolar disorder
(2023)
Journal Article
Health Inequality and its link to HbA1c Test Recovery in a Developed Health Economy: In a 'Nearly Post COVID-19' World
(2022)
Presentation / Conference
About Keele Repository
Administrator e-mail: research.openaccess@keele.ac.uk
This application uses the following open-source libraries:
Apache License Version 2.0 (http://www.apache.org/licenses/)
Apache License Version 2.0 (http://www.apache.org/licenses/)
SIL OFL 1.1 (http://scripts.sil.org/OFL)
MIT License (http://opensource.org/licenses/mit-license.html)
CC BY 3.0 ( http://creativecommons.org/licenses/by/3.0/)
Powered by Worktribe © 2025
Advanced Search